Hi, I'm Shrav, a
Multidisciplinary
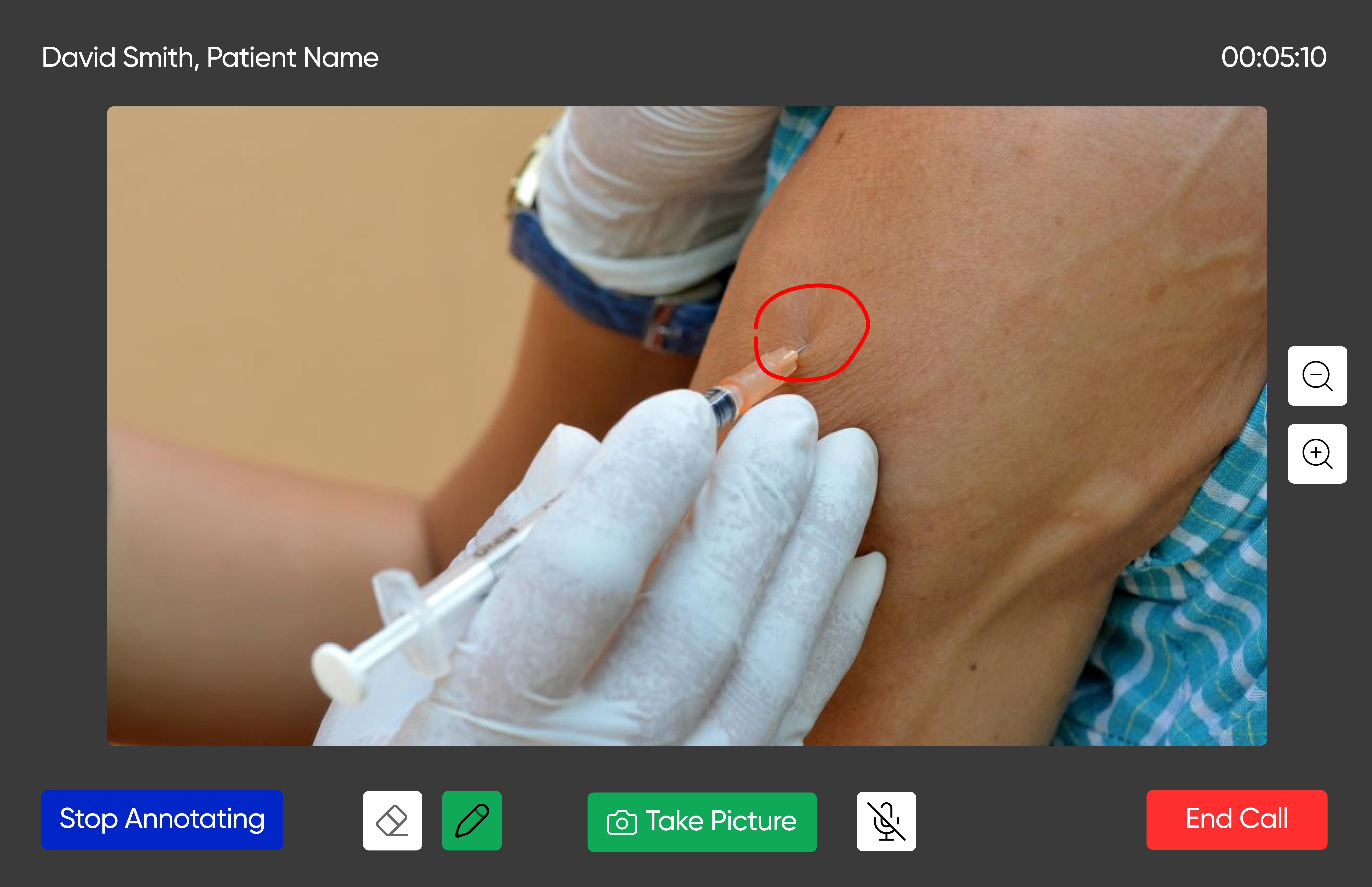
UX designer with a research-first practice, 2 years across AR telehealth, social commerce, and accessibility design.
designerWho I am
UX and brand designer. I care about edge cases, accessibility, and the users no one modelled.
Background
I love questioning briefs and over-indexing on research, trying to understand what is actually being solved before touching Figma.
I don't start with inspiration. I start with flow.
ദ്ദി˶ᵔ ᵕ ᵔ˶) designer ♡
श्रावणी
The brief might be right. It might be wrong. Research is how I tell the difference.
My design philosophy
My Case Studies

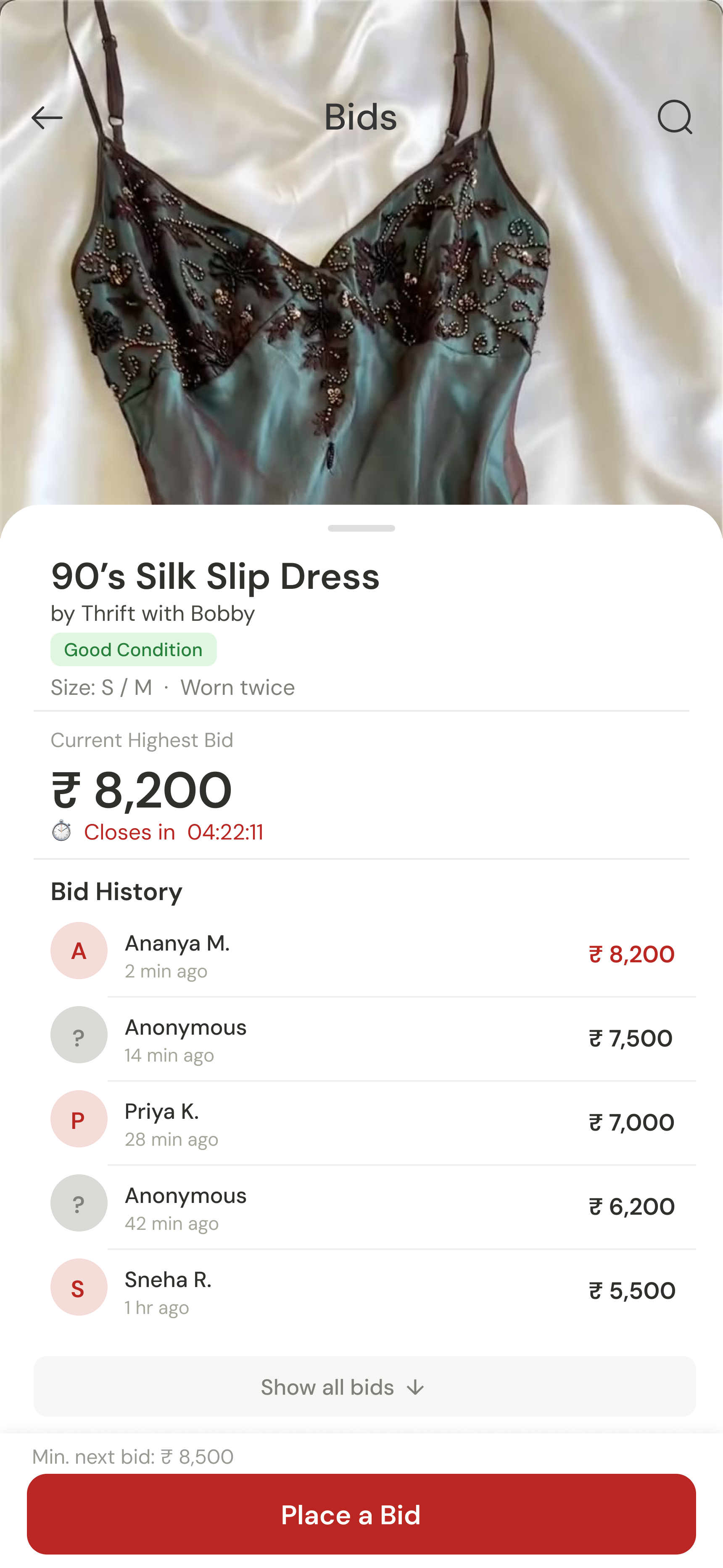
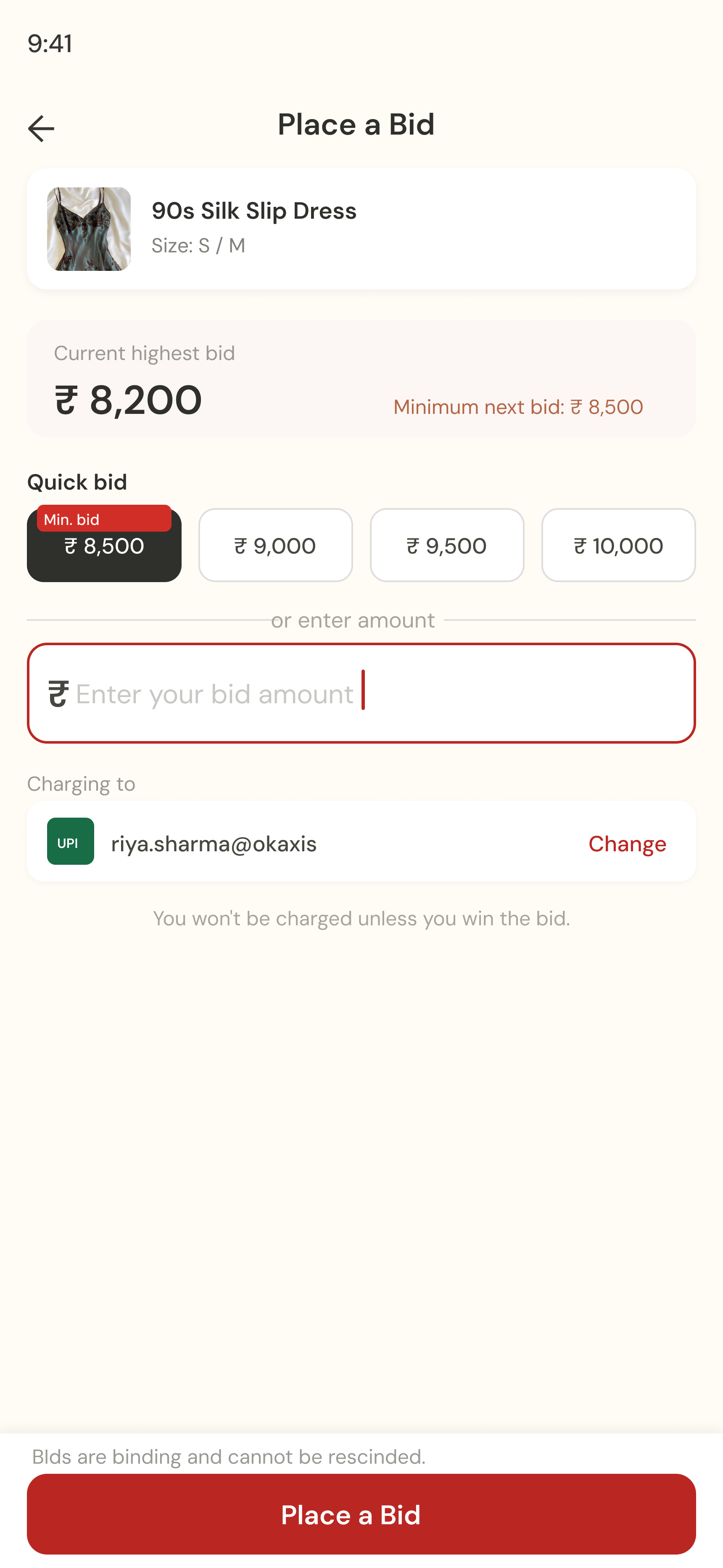
Brand + Product · Commercial Project
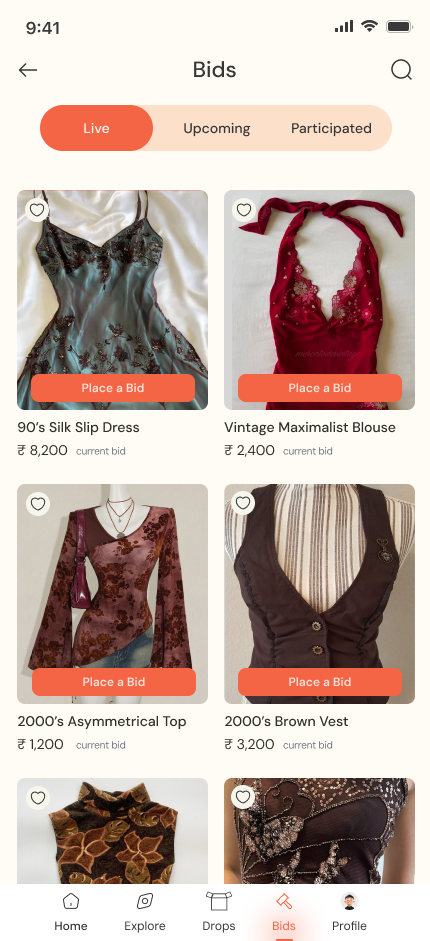
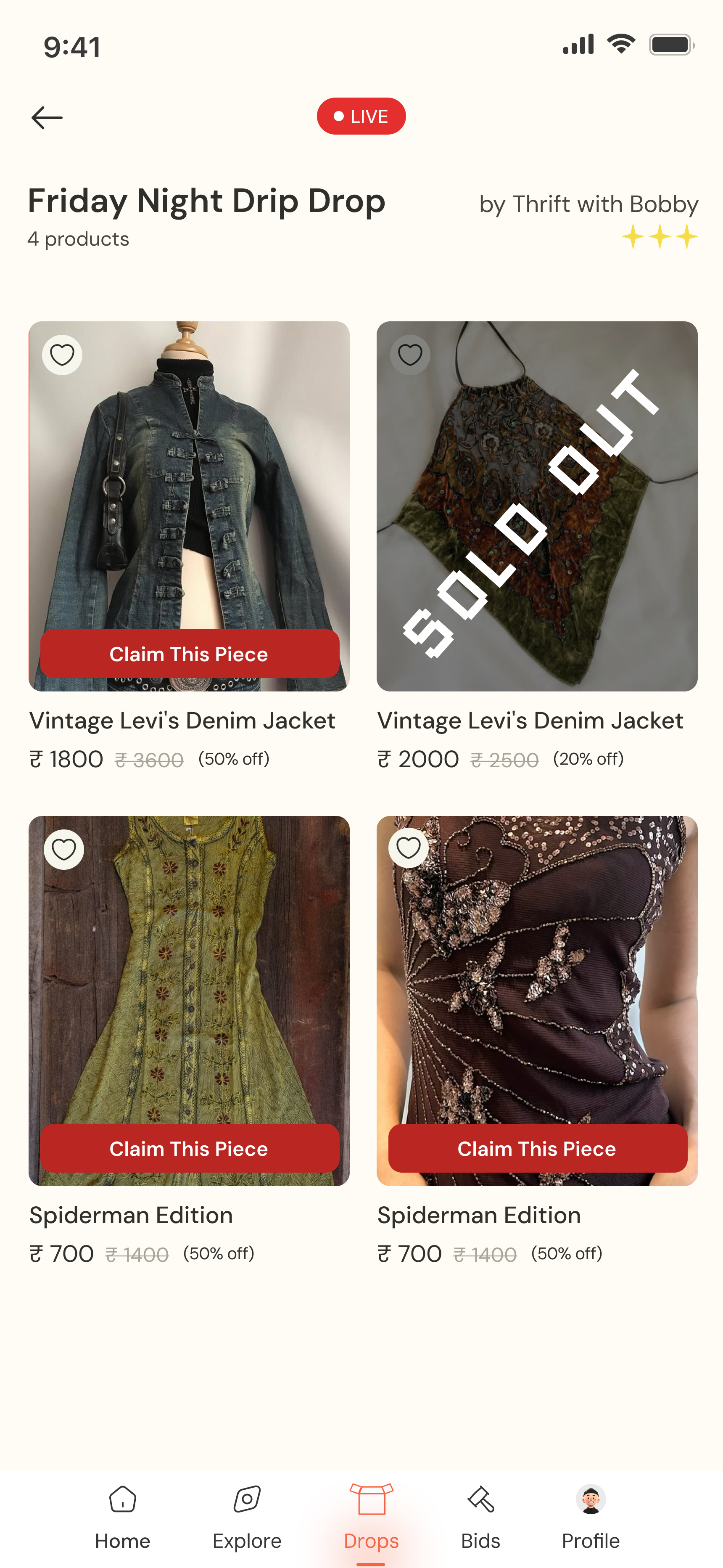
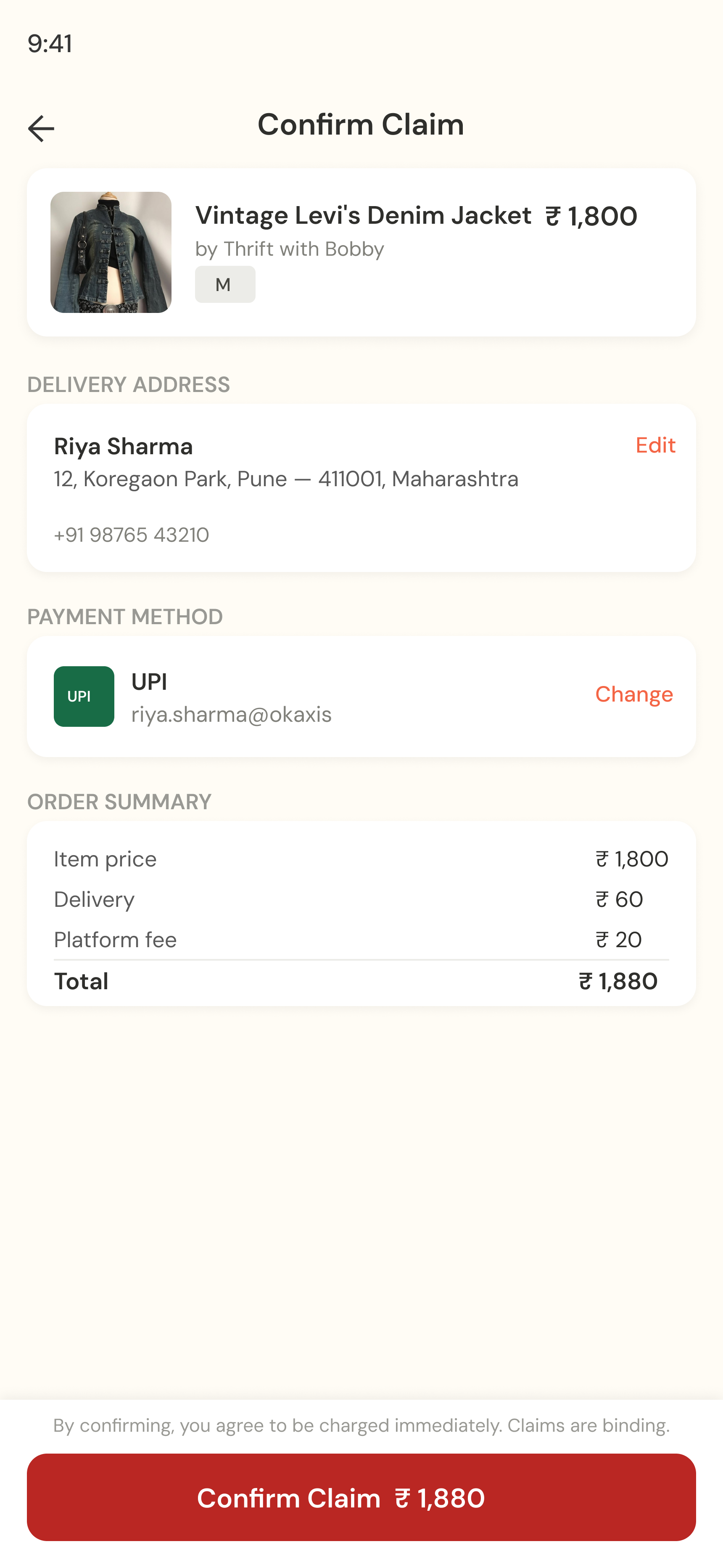
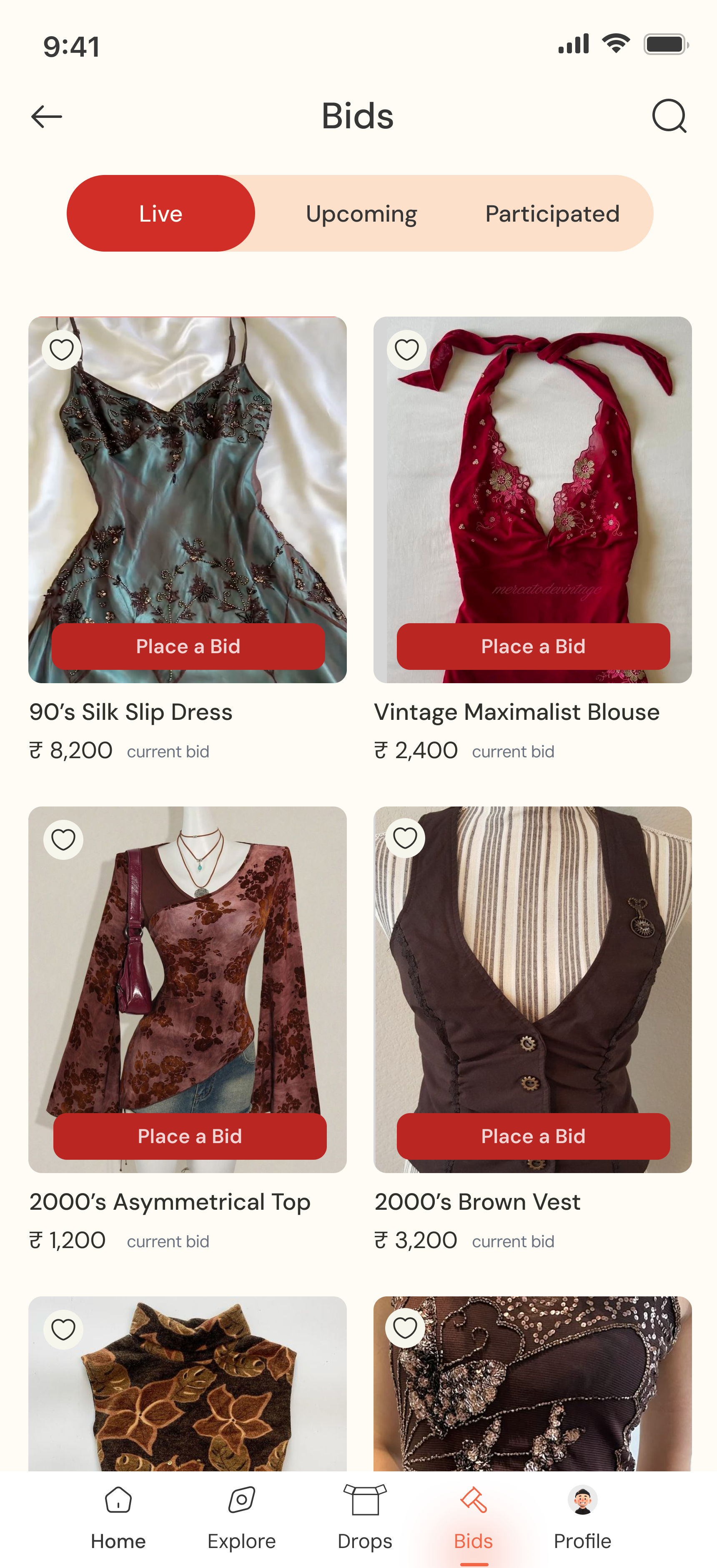
Thrift My Drip →
Brand identity and product design for a resale app built around the way Indian thrift actually works, drops, reels, and DMs.

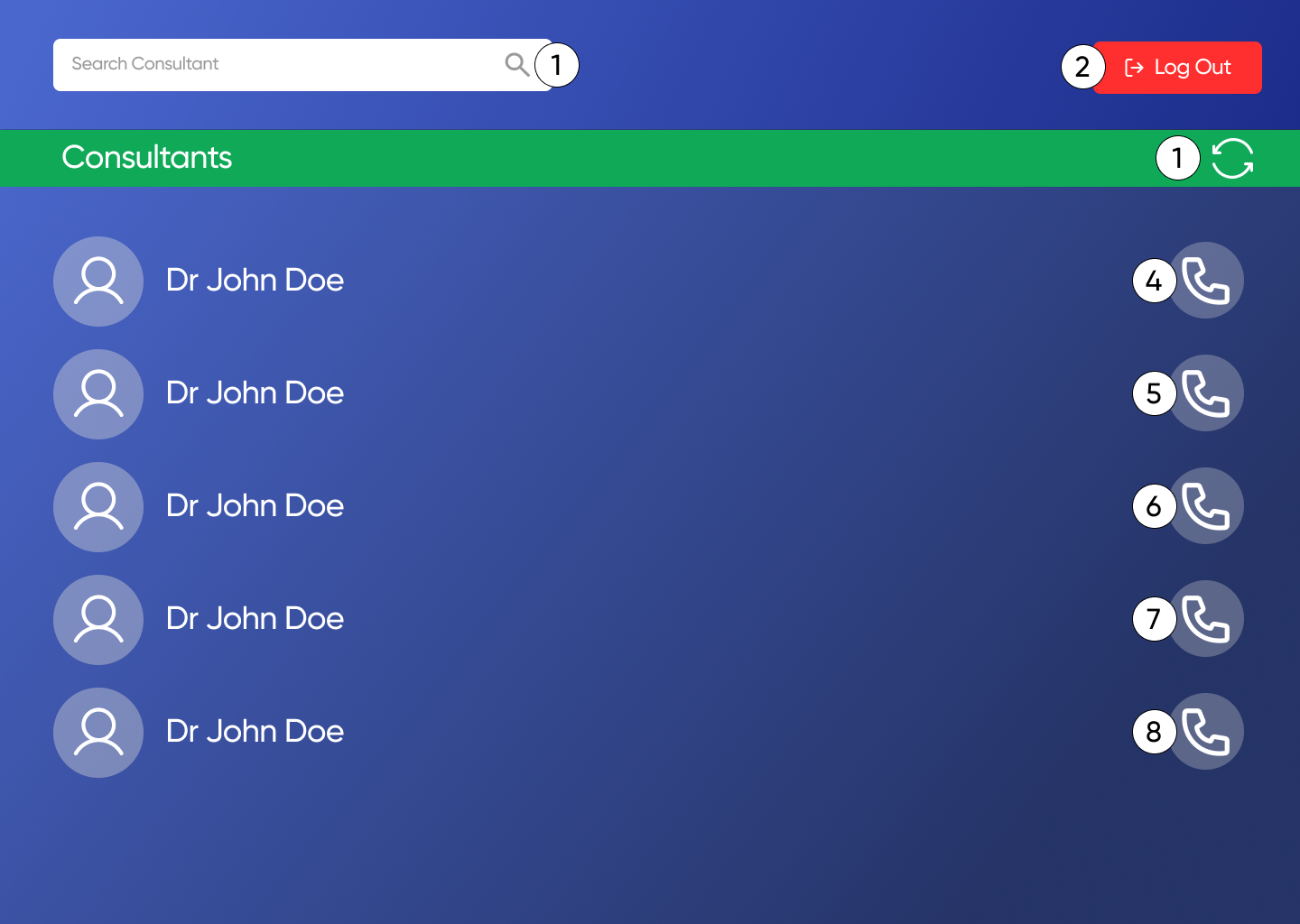
UX · Commercial Project
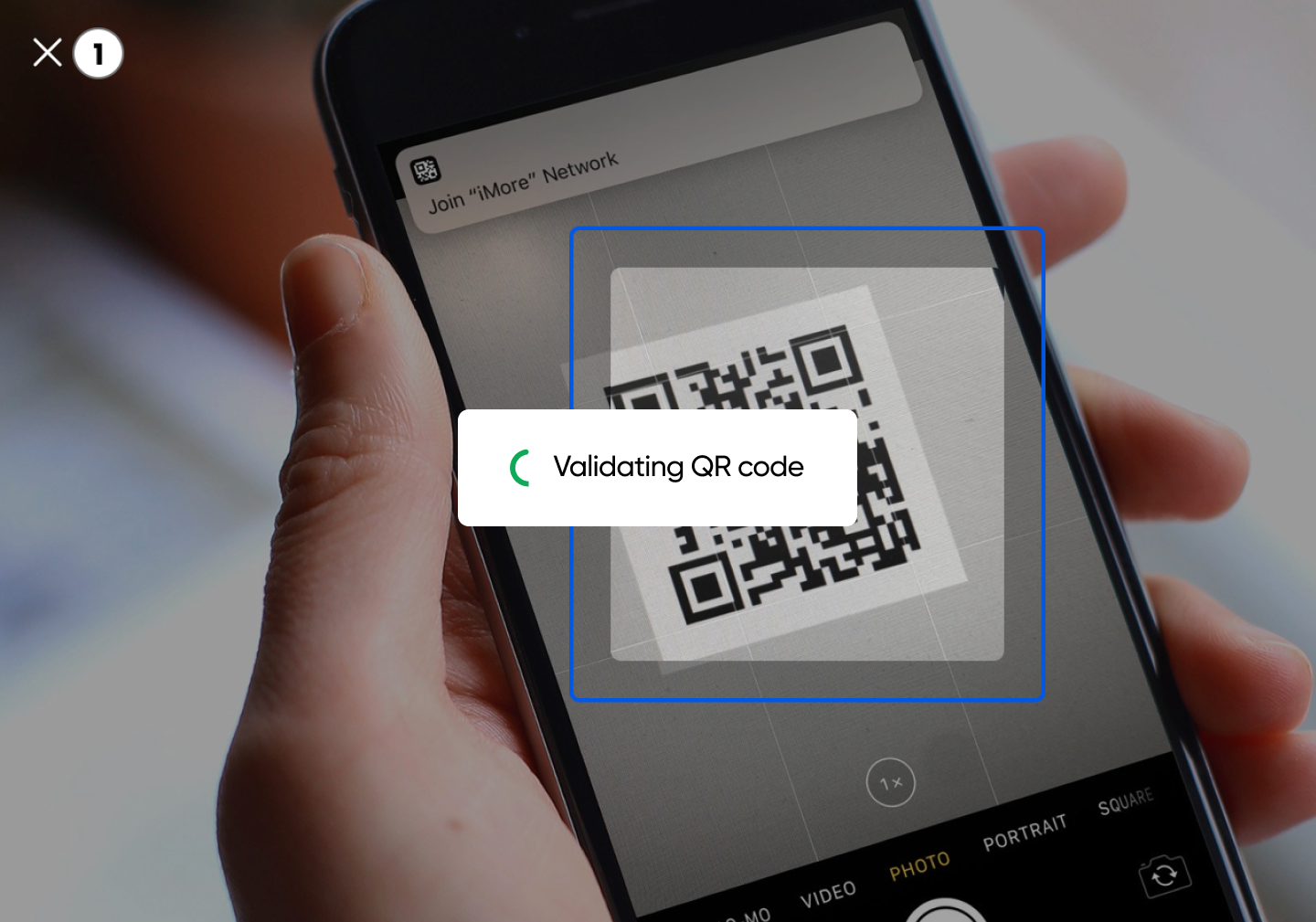
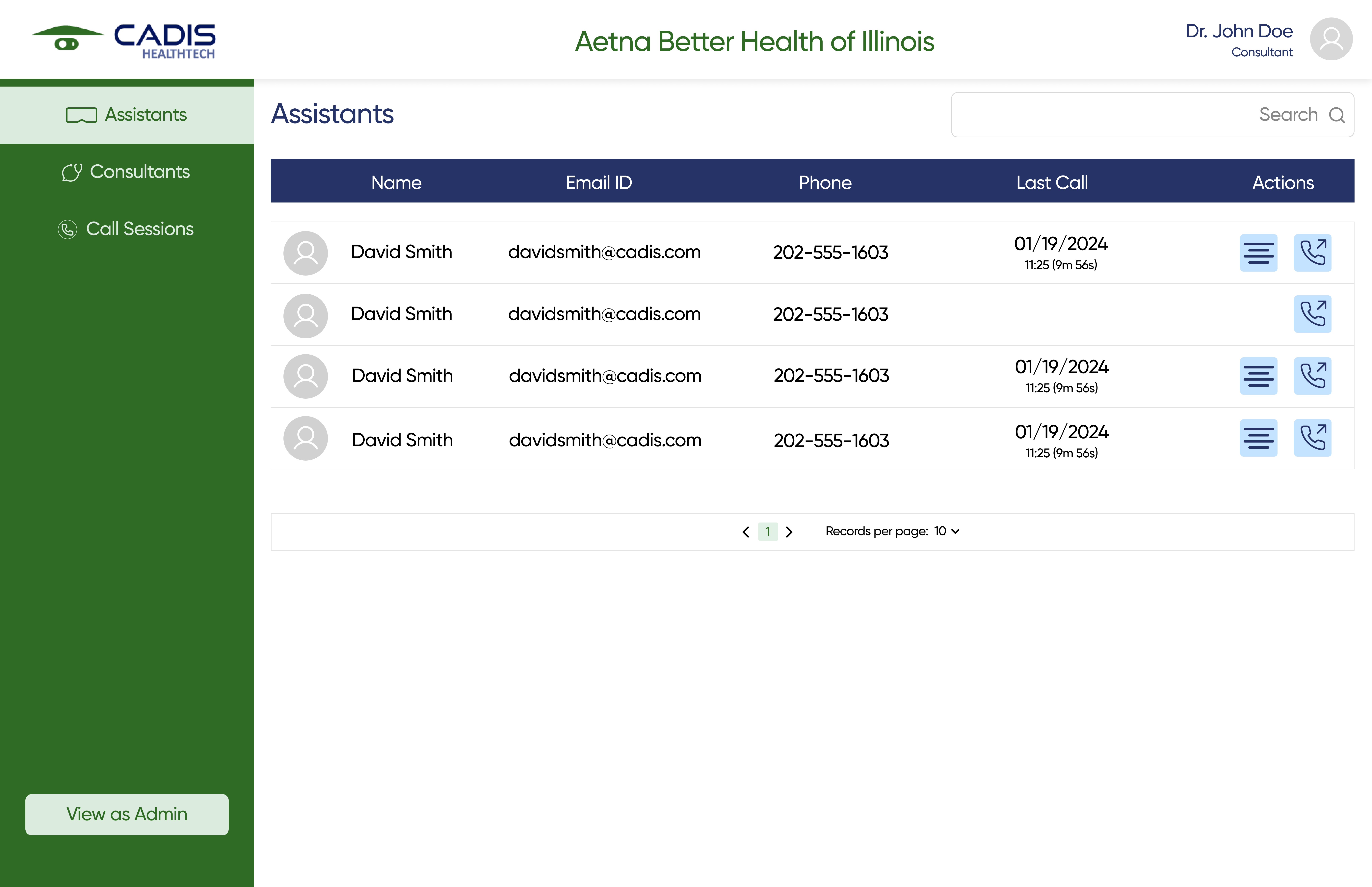
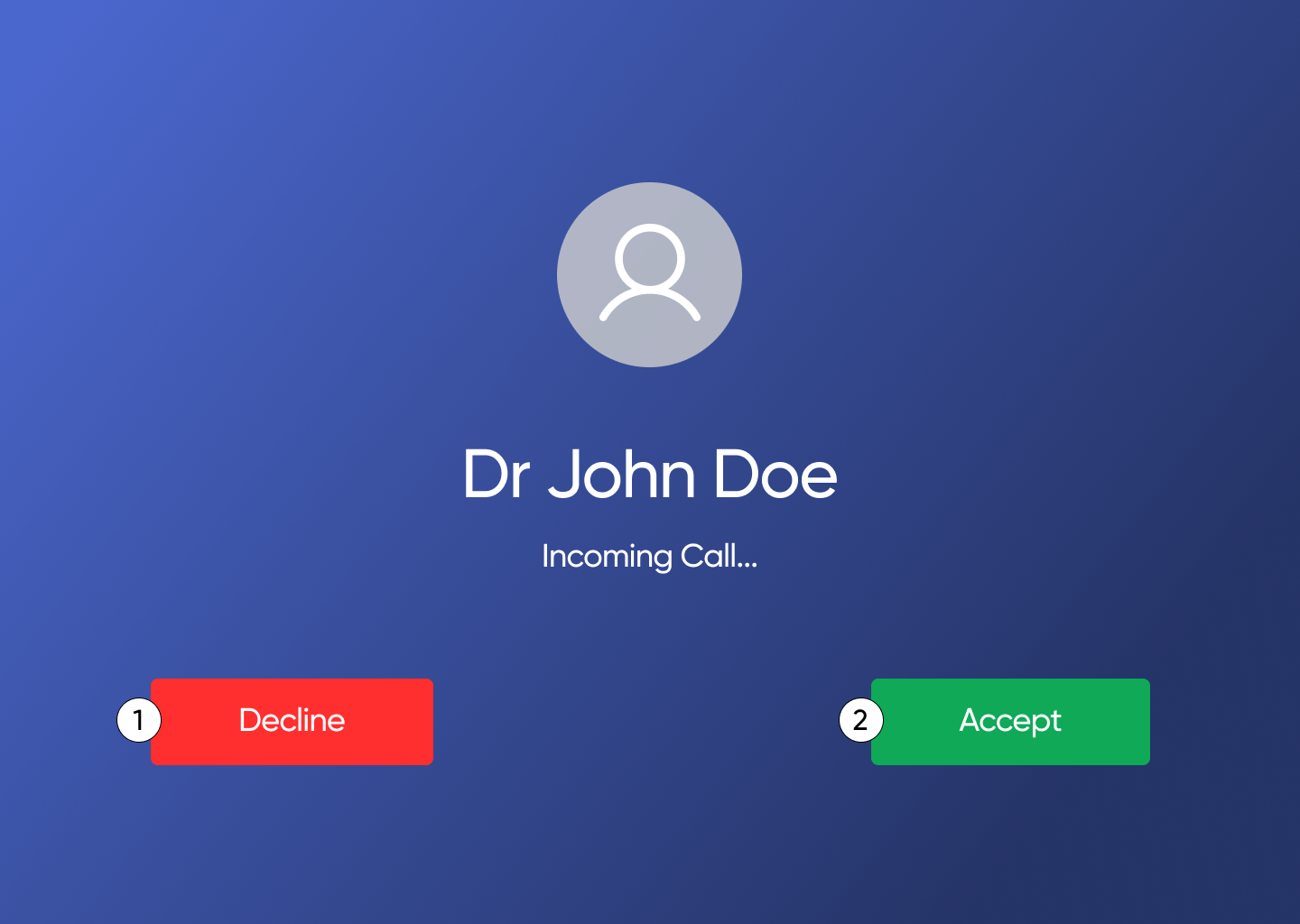
Cadis EziExpert →
I joined a live commercial product mid-build as the only UX designer. Audited, designed, shipped.

Thesis · Concept Project
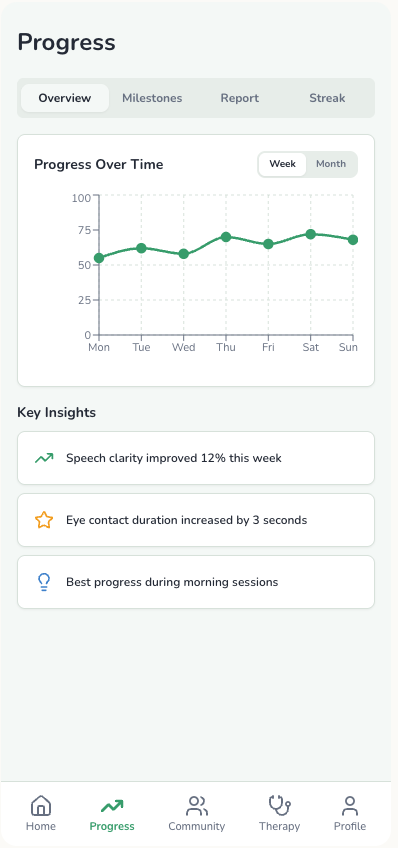
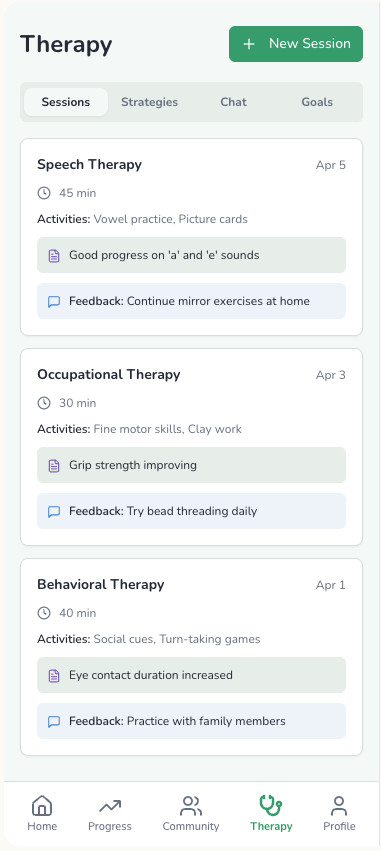
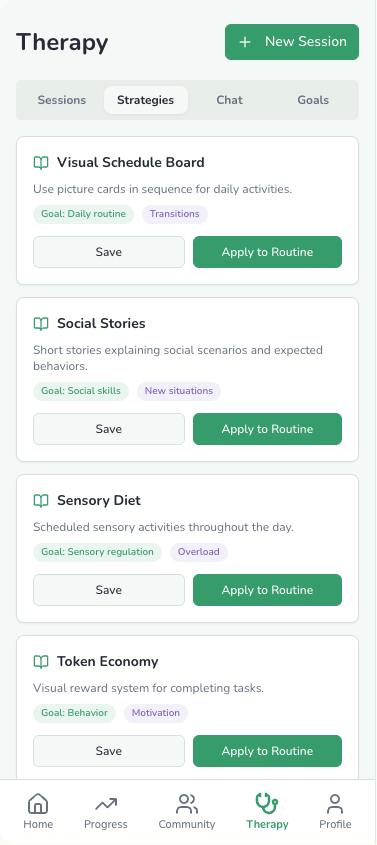
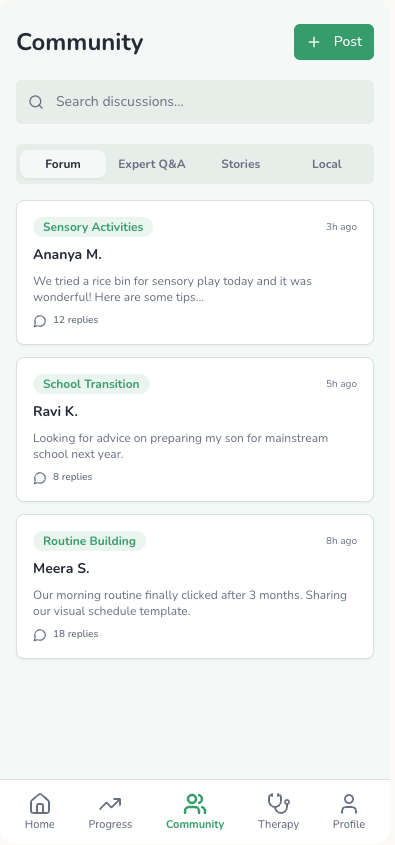
AutiMate →
Accessibility design. Started with the wrong user, research proved it, and I changed the brief.

UX + Research · Commercial Project
TenderGenie →
Research and interface design for an AI tendering tool, helping EPC and engineering teams cut through RFP complexity faster.
If you're building something and need a designer who can work from brand to shipped product, let's talk!
build together?
Get talking →